Infiltración Osea en Consulta Ambulatoria (Bone Infiltration in Ambulatory Consultation)
I have been working and using the biological-regenerative treatment called plasma rich in growth factors for more than 10 years.
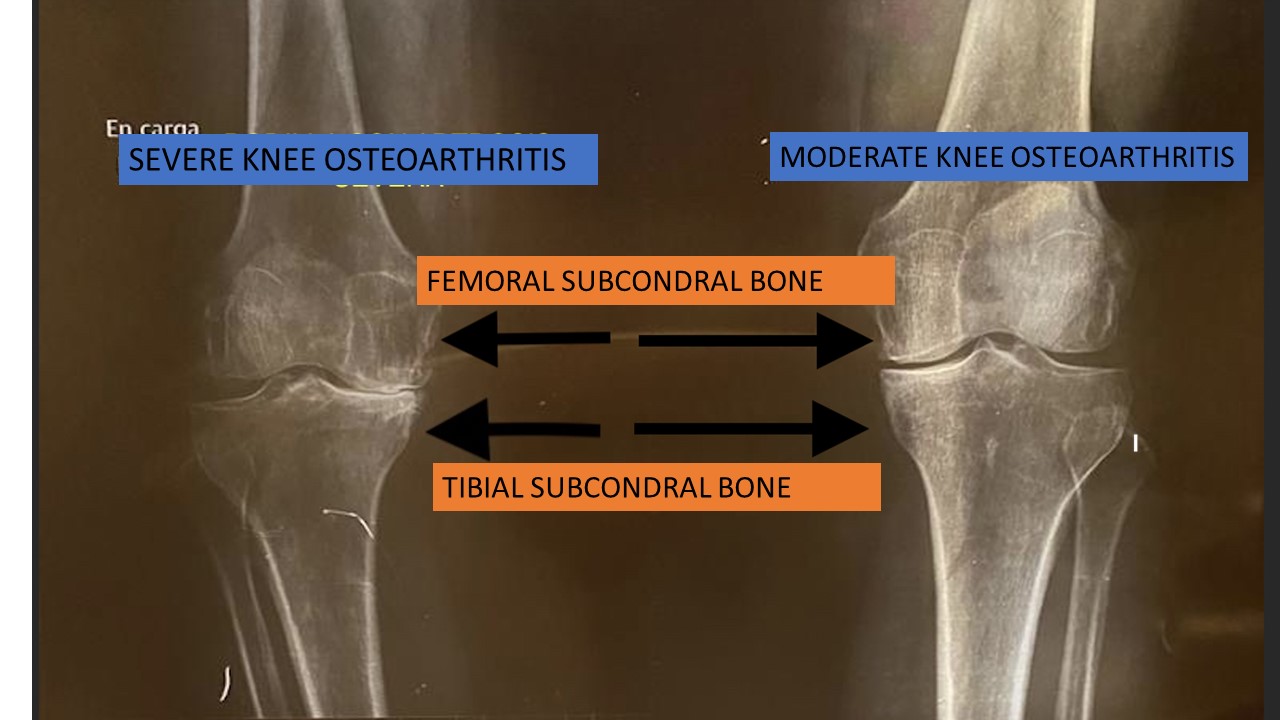
Osteoarthritis is one of the battlefields where this biological treatment has a greater prestige. Intra-articular injections are usually used and the plasma is infiltrated INSIDE the joint, be it hip, knee or ankle. For years, attention has been paid to another aspect of the joints: the subchondral bone. It is the bone that is covered by the layer of cartilage in the joints. When the cartilage dies, the underlying bone is exposed and pain sets in.
The subchondral bone is fundamental. It is responsible for absorbing between 50-60% of the weight that a joint is capable of supporting. It is like the concrete that supports the walls of the house and the cartilage is the facade of the house. There is direct communication between the cartilage and the subchondral bone through channels. In addition, abundant stem cells, also called mesenchymal cells, are located in subchondral bone, which are the ones that become healthy cells that replace the sick or old ones.
In osteoarthritis, an increase in communication channels between the cartilage and the underlying subchondral bone has been observed. In addition, stem cells function irregularly and have genetic abnormalities. If we treat the subcondral bone, we will be able to benefit the cartilage that covers said bone and that is found in the joints. We will also improve the function of stem cells. This has been widely confirmed in numerous studies in which better results have been seen when the joint is infiltrated and the subchondral bone is also «perforated» than when the joint is infiltrated alone.
We have developed a WORLDWIDE PIONEERING, PAINLESS AND OUTPATIENT way of introducing plasma into the subchondral bone, in any joint with osteoarthritis. At the present time we have used it on the knee, hip, shoulder, ankle and foot.
The results are incredible, relieving pain and recovering the function of the arthritic joint.
IT IS NOT NECESSARY TO DO IT IN THE OPERATING ROOM
To date, to treat subchondral bone, perforations have been made using a high-speed trocar (it is similar to a drill and is used to take bone biopsies) after locating the site to be infiltrated with an X-ray device and sedation to avoid the pain. Everything is done in the operating room.
This is going to change from now on, thanks to a type of local anesthesia called WALANT. It is performed by infiltrating local anesthesia (Lidocaine, Adrenaline) in the area to be infiltrated. Lidocaine is a very powerful anesthetic and adrenaline prevents bleeding after drilling the bone*. It allows procedures to be carried out on many occasions with a reduction in the risks derived from anesthesia (nausea, vomiting, discharge delay, prolonged motor blockade, sedation…), and in which, as there is no motor blockade** (it does not affect leg strength, sensation only) the patient can go home on the fly. But the most important thing is that it can be done in the consultation, IT IS NOT NECESSARY TO DO IT IN THE OPERATING ROOM.

**What does it mean that there is no motor block?
If traditional anesthesia is infiltrated by puncturing the patient’s armpit or hamstring, a sensory block is produced (he does not feel any pain) but also a motor block (he cannot move his hand or foot) during the time it takes for the body to metabolize said anesthesia, which can be hours. With WALANT, the type of anesthesia is only sensitive, that is, the patient does not notice any pain but can move the hand or foot, since there is no motor block and they are awake since it is a local anesthesia.
*No bleeding?
Through the use of adrenaline in the surgical field, we achieve an area of reversible ischemia, that is, the wound does not bleed for hours, which is the time that its effect lasts, and we avoid the use of the ischemia tourniquet and the associated sedation. The combination of a local anesthetic with adrenaline allows us to perform perforations without pain or bleeding with a fully awake and cooperative patient.
This system is called the INOCA PROTOCOL. They are the acronyms corresponding to Bone Infiltration in Ambulatory Consultation.
The first results have been presented at TOBI 2022 in Miami (World Orthobiology Symposium), where it has had a fantastic reception.

The INOCA technique has been published by the journal ARTHROSCOPY TECHNIQUES, recognizing its innovative nature and the usefulness it represents.

With Dr. Sampson, President of the Miami 2022 Congress
STEPS TO FOLLOW FOR THE INOCA TECHNIQUE

By using the ultrasound machine we can clearly and safely visualize the entry points where the bone is going to be drilled.
.



After treatment, the patient goes home without any problem. You can drive and for discomfort after the procedure, paracetamol 1 gram every 8 hours is sufficient..
Patient recording the procedure herself.
Absolute absence of pain.
Results three months later


Patient testimonial about INOCA treatment
Performing movements that before the treatment you could not do
What will INOCA mean?
Well, many patients who had to be taken to the operating room to perform the complete procedure (joint infiltration and perforation of the subchondral bone), can now be performed in the office itself and on an outpatient basis. Pain control is total, there is no bleeding and there is no post-infiltration pain.
It is indicated for patients with hip or knee osteoarthritis, advanced stages (grade 3 and 4).
We also do it on the shoulder, ankle and foot.
How many times do I have to infiltrate?
There are three sessions performed every 7 days, so the treatment is completed after 21 days.
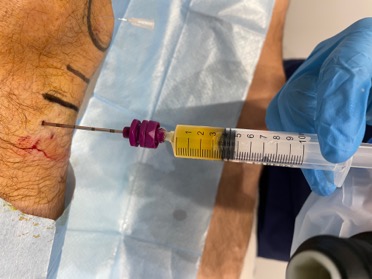
In each session an infiltration is carried out inside the joint as well as a bone perforation of both the femur and the tibia, thus treating the subchondral bone that plays such an important role in osteoarthritis pain. Everything is done under local anesthesia and with all the aseptic measures that the procedure requires.
Once the infiltration is finished, the patient leaves without the need to remain under observation.
For possible discomfort once the anesthesia has been metabolized, paracetamol or metamizol is enough.